
Wednesday, December 21, 2016
Monday, December 19, 2016
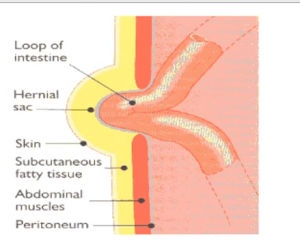
Brief Description Of Abdominal Wall Hernias
Abdominal wall hernias:
Definition: The classical surgical definition of a hernia is the protrusion of an organ or the fascia of an organ through the wall of the cavity that normally contains it.

Risk factors for abdominal wall hernias include:
Clinical Features include:
Types of abdominal wall hernias:
1. Inguinal hernia:

Definition: The classical surgical definition of a hernia is the protrusion of an organ or the fascia of an organ through the wall of the cavity that normally contains it.
Risk factors for abdominal wall hernias include:
- obesity
- ascites
- increasing age
- surgical wounds
Clinical Features include:
- a palpable lump
- cough impulse
- pain
- obstruction: more common in femoral hernias
- strangulation: may compromise the bowel blood supply leading to infarction
Types of abdominal wall hernias:
1. Inguinal hernia:
- Inguinal hernias account for 75% of abdominal wall hernias.
- Around 95% of patients are male; men have around a 25% lifetime risk of developing an inguinal hernia.
- Above and medial to pubic tubercle Strangulation is rare

2. Femoral hernia:
Friday, December 9, 2016



Sunday, December 4, 2016
Toxic Epidermal Necrolysis

Toxic epidermal necrolysis (TEN) is a potentially lifethreatening skin disorder that is most commonly seen secondary to a drug reaction.
In this condition the skin develops a scalded appearance over an extensive area. Some authors consider TEN to be the severe end of a spectrum of skin disorders which includes erythema multiforme and Stevens Johnson syndrome
Clinical Features
- systemically unwell e.g. pyrexia, tachycardic
- positive Nikolsky's sign: the epidermis separates with mild lateral pressure
Drugs known to induce Toxic epidermal necrolysis (TEN)
Tuesday, November 29, 2016
A Child Presents With A Skin Lesion With No Other Associated Symptoms.
A 6-year-old child presents with the skin lesions shown below:

The lesions have been present over the last month, and the child has reported no symptoms associated with them. The most likely diagnosis is
A) Varicella
B) Herpes zoster
C) Rhus dermatitis
D) Molluscum contagiosum
E) Scabies
The answer is

The lesions have been present over the last month, and the child has reported no symptoms associated with them. The most likely diagnosis is
A) Varicella
B) Herpes zoster
C) Rhus dermatitis
D) Molluscum contagiosum
E) Scabies
The answer is
Monday, November 28, 2016


Saturday, November 26, 2016
Athlete's Foot Or Tinea Pedis

Athlete's foot is also known as tinea pedis. It is usually caused by fungi in the genus Trichophyton and affects the skin on the feet.
Athlete's foot is one of the most common fungal skin infections.
Athlete's foot fungus may infect any part of the foot, but most often grows between the toes.
Causes And Risk Factors: Athlete's foot spreads easily. You can get it by touching the toes or feet of a person who has it. But most often, people get it by walking barefoot on contaminated surfaces near swimming pools or in locker rooms. The fungi then grow in the shoes, especially if the shoes are so tight that air cannot move around the feet.
Risk factors for getting infected with Athlete's foot are:
- Male gender
- People who frequently wear damp socks or tight fitting shoes
- Sharing mats, rugs, bed linens, clothes or shoes with someone who has a fungal infection
- Walking barefoot in public areas where the infection can spread, such as locker rooms, swimming pools, communal baths and showers.
Clinical Features: Athlete's foot usually causes a scaly red rash.
Friday, November 25, 2016





Thursday, November 24, 2016

Actinic keratoses - Brief Discussion

Actinic, or solar, keratoses (AK) is a rough, scaly patch on the skin and is a common premalignant lesion that develops as a consequence of chronic sun exposure. It's most commonly found on your face, lips, ears, back of your hands, forearms, scalp or neck.
Clinical Features:
- small, crusty or scaly, lesions
- may be pink, red, brown or the same color as the skin
- typically on sun exposed areas e.g. temples of head
- multiple lesions may be present
Risk Factors: include:
- Age older than 40
- Living in a sunny climate
- A history of frequent or intense sun exposure or sunburn
- Red or blond hair, and blue or light-colored eyes
Wednesday, November 23, 2016
Corneal Foreign Body and Corneal Abrasion
A 28-year-old man felt something fly into his eye while he was using a table saw without wearing protective eye gear. He presented with pain, tearing, photophobia, and thought that something was still in his eye.
On examination with a slit lamp, the physician noted that he had a wood chip that had penetrated the cornea (See pictures below)
 Wood chip is visible in the cornea on close inspection of the eye.
Wood chip is visible in the cornea on close inspection of the eye.
\
 Slit-lamp examination reveals this wood chip has penetrated the cornea.
Slit-lamp examination reveals this wood chip has penetrated the cornea.
He was referred to an ophthalmologist who successfully removed the foreign body. He was treated with a short course of topical NSAIDs for pain relief, and had complete healing.
Case Discussion:
Corneal Foreign Body and Corneal Abrasion
Introduction: Corneal abrasions are often caused by eye trauma and can cause an inflammatory response. Corneal abrasions are detected using fluorescein and a UV light. A corneal foreign body can be seen during a careful physical examination with a good light source or slit lamp.
Nonpenetrating foreign bodies can be removed by an experienced physician in the office using topical anesthesia. Refer all penetrating foreign bodies to an ophthalmologist.
Pathophysiology: The cornea overlies the iris and provides barrier protection, filters UV light, and refracts light onto the retina.
• Abrasions in the cornea are typically caused by direct injury from a foreign body, resulting in an inflammatory reaction.
• The inflammatory reaction causes the symptoms and can persist for several days after the foreign object is out.
History and Physical Examination:
• History of ocular trauma or eye rubbing (although corneal abrasions can occur with no trauma history).
On examination with a slit lamp, the physician noted that he had a wood chip that had penetrated the cornea (See pictures below)

\

He was referred to an ophthalmologist who successfully removed the foreign body. He was treated with a short course of topical NSAIDs for pain relief, and had complete healing.
Case Discussion:
Corneal Foreign Body and Corneal Abrasion
Introduction: Corneal abrasions are often caused by eye trauma and can cause an inflammatory response. Corneal abrasions are detected using fluorescein and a UV light. A corneal foreign body can be seen during a careful physical examination with a good light source or slit lamp.
Nonpenetrating foreign bodies can be removed by an experienced physician in the office using topical anesthesia. Refer all penetrating foreign bodies to an ophthalmologist.
Pathophysiology: The cornea overlies the iris and provides barrier protection, filters UV light, and refracts light onto the retina.
• Abrasions in the cornea are typically caused by direct injury from a foreign body, resulting in an inflammatory reaction.
• The inflammatory reaction causes the symptoms and can persist for several days after the foreign object is out.
History and Physical Examination:
• History of ocular trauma or eye rubbing (although corneal abrasions can occur with no trauma history).
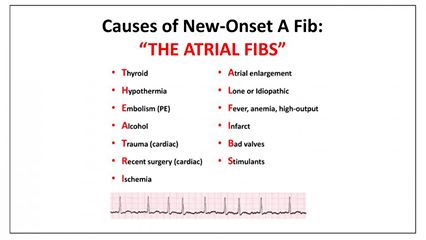
A 42-year-old woman presents to the emergency room complaining of shortness of breath and palpitations.
A 42-year-old woman presents to the emergency room complaining of shortness of breath and palpitations. An electrocardiogram shows the tracing shown below.
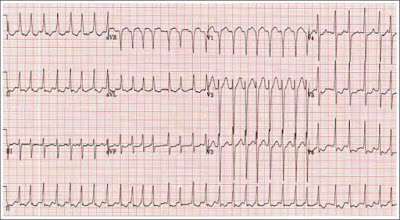
Appropriate management at this time includes
A) Epinephrine
B) Metoprolol
C) Nitroglycerin
D) Adenosine
E) Lidocaine
Answer:

Appropriate management at this time includes
A) Epinephrine
B) Metoprolol
C) Nitroglycerin
D) Adenosine
E) Lidocaine
Answer:
Tuesday, November 22, 2016



Monday, November 21, 2016
Angioedema And Hereditary angioedema (HAE)
Regarding Angioedema answer the following questions:
1. What are the clinical pictures associated w ith angioedema?
2. What pathophysiologic processes underlie angioedema?
3. How is hereditary angioedema (HAE) diagnosed?

Answers:
1. What are the clinical pictures associated w ith angioedema?
2. What pathophysiologic processes underlie angioedema?
3. How is hereditary angioedema (HAE) diagnosed?

Answers:
A Brief Description Of Acne Rosacea

Acne rosacea is a chronic skin disease of unknown aetiology
Clinical Features
- typically affects nose, cheeks and forehead
- flushing is often first symptom
- telangiectasia are common
- later develops into persistent erythema with papules and pustules
- rhinophyma
- ocular involvement: blepharitis

Stages And Types Of Rosacea:



Saturday, November 19, 2016
Regarding Frozen Shoulder (Adhesive Capsulitis)

Which of the following diseases is associated with frozen shoulder (adhesive capsulitis)?
A. Diabetes mellitus
B. Osteoarthritis
C. Hypertension
D. Pregnancy
E. Gout
Answer
Answer
Acanthosis Nigricans And Associated Medical Conditions.

You note the above skin disorder during a general medical evaluation. You explain to the patient they are at risk for the development of
A) Alzheimer’s disease
B) Tuberculosis
C) Diabetes mellitus
D) Graves’ disease
E) Melanoma
Answer And Discussion:
Thursday, November 17, 2016



Differential Diagnosis Of Normal Pressure Hydrocephalus (NPH)
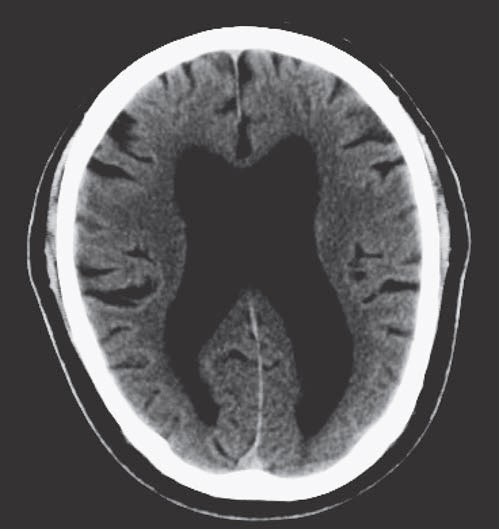
Normal Pressure Hydrocephalus (NPH) can be idiopathic or secondary to meningitis, subarachnoid hemorrhage, or head trauma, and is caused by impaired reabsorption of spinal fluid. Patients present with gait abnormalities, urinary
incontinence, and/or cognitive impairment. Diagnosis is confirmed by radiographic evidence and a normal opening pressure on lumbar puncture.
Differential Diagnosis:
• Alzheimer disease—Impaired orientation and memory, which are often spared in NPH; cortical atrophy.
A 60-year-old retired construction worker presents with a non-healing skin lesion on his face
A 60-year-old retired construction worker presents with a non-healing skin lesion on his face that occasionally bleeds when he gets out of the shower. The picture in closeup of the lesion is shown below:

The most likely diagnosis is
A) Basal cell carcinoma
B) Squamous cell carcinoma
C) Superficial spreading malignant melanoma
D) Actinic keratosis
E) Keratoacanthoma
Answer:

The most likely diagnosis is
A) Basal cell carcinoma
B) Squamous cell carcinoma
C) Superficial spreading malignant melanoma
D) Actinic keratosis
E) Keratoacanthoma
Answer:
Wednesday, November 16, 2016
A 68 Year Old Man, A Retired Fire Man Presents With Symptoms Of Lower Chest Infection
A 68-year-old man, a retired fireman, has developed symptoms of lower respiratory chest infection,
which have left him with a hacking cough. His CXR is shown below:

What would you arrange next to establish the diagnosis?
A A trial of inhaled corticosteroids
B Full lung function tests
C Fibreoptic bronchoscopy
D High-resolution CT chest scan
E Echocardiogram
Answer:
which have left him with a hacking cough. His CXR is shown below:

What would you arrange next to establish the diagnosis?
A A trial of inhaled corticosteroids
B Full lung function tests
C Fibreoptic bronchoscopy
D High-resolution CT chest scan
E Echocardiogram
Answer:


Tuesday, November 15, 2016
Club Foot Deformity - A Brief Discussion

Clubfoot describes a range of foot abnormalities usually present at birth (congenital) in which the foot is twisted out of shape or position.
Also known as talipes equinovarus.
In patients with a club foot any of the following characteristics may be present, and each may vary from mild to severe:
- The foot (especially the heel) is usually smaller than normal.
- The foot may point downward.
- The front of the foot may be rotated toward the other foot.
- The foot may turn in, and in extreme cases, the bottom of the foot can point up.
A club foot may occur as an isolated feature or, with multiple malformations else where but is usually an isolated problem for an otherwise healthy newborn.
Etiology: The cause of clubfoot is unknown (idiopathic), but it may be a combination of genetics and environment. Certain risk factors like family history, smoking in mother during pregnancy and decreased amniotic fluid may contribute to having club foot in the baby.
Clinical Features: Clubfoot typically doesn't cause any problems until the child starts to stand and walk. Although clubfoot is painless in a baby, treatment should begin immediately. Clubfoot can cause significant problems as the child grows. But with early treatment most children born with clubfoot are able to lead a normal life.
Complications: Untreated club foot can cause serious complications like:


Monday, November 14, 2016
A 45-year-old woman presents with a localized area of erythematous scaly patches that comes and goes and typically affects the elbows
A 45-year-old woman presents with a localized area of erythematous scaly patches that comes and goes and typically affects the elbows. ( Picture shown below) The likely diagnosis is
A) Pityriasis rosacea
B) Mycosis fungoides
C) Tinea corpora
D) Nummular eczema
E) Psoriasis

Answer And Discussion:
A) Pityriasis rosacea
B) Mycosis fungoides
C) Tinea corpora
D) Nummular eczema
E) Psoriasis

Answer And Discussion:
Subscribe to:
Posts (Atom)