referred to as the “gate-keeper to the fetus.” Careful examination of the placenta, its membranes,
and the umbilical cord can prove to be a valuable aid in the diagnosis and treatment of the
neonate. Gross examination of the placenta takes five minutes, and more sophisticated examination
should be considered when there is poor pregnancy outcome, recognizable malformations or
abnormalities, multiple gestation, extremes of amniotic fluid volume, severe intrauterine growth
retardation, short umbilical cord (< 32 cm), and profound acidemia.
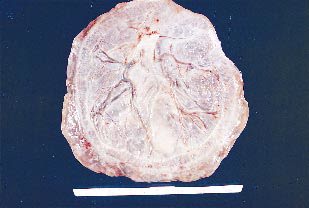
The maternal surface of the placenta (decidual plate) is soft, spongy and dark red; and the fetal surface (chorionic plate) is shiny and steel blue to gray.
The placenta, membranes, and umbilical cord weigh approximately 400 to 600 g at birth.
Abnormalities in structure can result in an inefficient transport of oxygen and nutrients to the developing baby. Despite this importance, it is one of the least understood and investigated human organs.


are of nearly equal size and this occurs in about 1% of deliveries. Note that the lobes are separated by membranes. The umbilical cord may insert into one or other lobe, or may insert between the two.