These disorders generally produce fatal bleeding or infection, particularly when they’re idiopathic or stem from the use of chloramphenicol or from infectious hepatitis. Mortality for patients who have aplastic anemia with severe pancytopenia is 80% to 90%.
Causes
Aplastic anemias usually develop when damaged or destroyed stem cells inhibit red blood cell (RBC) production. Less commonly, they develop when damaged bone marrow microvasculature creates an unfavorable environment for cell growth and maturation. About half of such anemias result from drugs (antibiotics, anticonvulsants), toxic agents (such as benzene and chloramphenicol), or radiation. The rest may result from immunologic factors (unconfirmed), severe disease (especially hepatitis), or preleukemic and neoplastic infiltration of bone marrow.
Idiopathic anemias may be congenital and account for about 50% of all confirmed occurrences. Two such forms of aplastic anemia have been identified: congenital hypoplastic anemia (Blackfan-Diamond anemia), which develops between ages 2 months and 3 months, and Fanconi’s syndrome, which develops between birth and age 10.
With Fanconi’s syndrome, chromosomal abnormalities are typically associated with multiple congenital anomalies—such as dwarfism and hypoplasia of the kidneys and spleen. In the absence of a consistent familial or genetic history of aplastic anemia, researchers suspect that these congenital abnormalities result from an induced change in the development of the fetus.
Signs and symptoms
Signs and symptoms of aplastic anemias vary with the severity of pancytopenia but usually develop insidiously. These include progressive weakness and fatigue, shortness of breath, headache, pallor and, ultimately, tachycardia and heart failure. Thrombocytopenia leads to ecchymosis, petechiae, and hemorrhage, especially from the mucous membranes (nose, gums, rectum, and vagina) or into the retina or central nervous system. Neutropenia may lead to infection (with fever, oral and rectal ulcers, and sore throat) but without characteristic inflammation.
Diagnosis
Confirmation of aplastic anemia requires a series of laboratory tests:
- RBCs are usually normochromic and normocytic (although macrocytosis [larger-than-normal erythrocytes] and anisocytosis [excessive variation in erythrocyte size] may exist), with a total count of 1 million/µl or less. Absolute reticulocyte count is low.
- Serum iron level is elevated (unless bleeding occurs), but total iron-binding capacity is normal or slightly reduced. Hemosiderin is present, and tissue iron storage is visible microscopically.
- Platelet, neutrophil, and white blood cell counts fall.
- Coagulation test results (bleeding time), reflecting decreased platelet count, are abnormal.
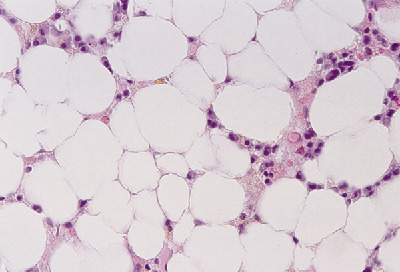
- Bone marrow aspiration from several sites may yield a “dry tap,” and a biopsy will show severely hypocellular or aplastic marrow, with varied amounts of fat, fibrous tissue, or gelatinous replacement; absence of tagged iron (because iron is deposited in the liver rather than in bone marrow) and megakaryocytes; and depression of erythroid elements.
Treatment
Identifiable causes must be eliminated and vigorous supportive measures must be provided, such as transfusions of packed RBCs and platelets. Human leukocyte antigen–matched leukocytes or antithymocyte globulin, used alone or in combination with cyclosporine, has especially impaired outcomes for children and severely neutropenic patients. Experimental trials of androgen therapy are in process. Even after elimination of the cause, recovery can take months. Bone marrow transplantation is the treatment of choice for patients with anemia resulting from severe aplasia and for patients who need constant RBC transfusions.
Preventing infection
Patients with low leukocyte counts need special measures to prevent infection. The infection itself may require specific antibiotics; however, they aren’t given prophylactically because they tend to encourage resistant strains of organisms. Patients with low hemoglobin (Hb) levels may need respiratory support with oxygen, in addition to blood transfusions.
Other treatments
Other appropriate treatments include a corticosteroid to stimulate erythroid production (tends to be successful in children but not adults); a marrow-stimulating agent, such as an androgen (which is controversial); an antilymphocyte globulin (which is experimental); an immunosuppressant (if the patient doesn’t respond to other therapy); and a colony-stimulating factor to encourage growth of specific cellular components.
I started on COPD Herbal treatment from Ultimate Health Home, the treatment worked incredibly for my lungs condition. I used the herbal treatment for almost 4 months, it reversed my COPD. My severe shortness of breath, dry cough, chest tightness gradually disappeared. Reach Ultimate Health Home via their website at www.ultimatelifeclinic.com I can breath much better and It feels comfortable!
ReplyDelete